
Aug 30, 2018
Evidence for the efficacy of Platelet Rich Plasma, a blood-derived formulation, and bone marrow derived biologics in osteoarthritis continues to grow in the orthopedic community. On the other hand, as I continually monitor the current landscape of indiscriminate and sometimes inappropriate marketing and use of biologics by the non-orthopedic opportunists, I doubt if the charlatans and camp followers have an overview of what is known about these agents. The increased presence of clinics Is driven by the popularity of PRP and its biologic cousins:
- consumer demand
- aggressive marketing
- a low regulatory bar for many of these regenerative medicine clinics
- the autologous nature that makes many approaches largely safe
- positive data from centers such as ours demonstrating functional and symptom modification
PRP works by activating cellular pathways; more than 3,000 genes are related to these and other pathways, suggesting that PRP probably acts by inducing a transitory inflammatory event, which then triggers tissue regeneration. Bone Marrow Concentrate, does more and addresses the subchondral bone when appropriately injected as well as initiate joint preservation and possible regeneration.
Taking aim
I use a hemoanalyzer to characterize a dose of PRP or Bone Marrow Concentrate allowing me to quantify the composition and biologic activity of these agents. Soon, I will begin pretreatment assessment of the synovial fluid of the arthritic joint so as to best determine who is the optimal candidate for a particular procedure
What do we know?
- Knee osteoarthritis: white blood cell-poor PRP has a positive effect on symptoms, not structure; while Bone marrow Concentrate affects symptoms and structure. I identify what I am putting into the patient. My goal is to have reliable predictors of outcome; that is, do the composition and biologic activity of the material implanted in the patient predict the clinical/imaging outcomes? My PRP contains a high concentration of anti-inflammatory cytokines and anabolic growth factors whereas my use of Bone Marrow Concentrate inside the bone adjacent to the joint in addition to the joint itself is improving the outcomes of the patients I treat.
- To learn more, call my office to schedule an appointment at (312) 475-1893
- You may view my Web site at WWW.Sheinkopmd.com
Tags: anit-inflammatory, biologics, bone marrow, cellular orthopedic, cellular therapy, cytokines, knee osteoarthritis, Orthopedic Surgeon, PRP, regenerative medicine, stem cell
Jul 19, 2018
The argument frequently advanced by orthopedic surgeons in response to a patient’s inquiry concerning stem cells for arthritis is that it is too early, there is not enough research, It is better to have a major surgical procedure. For those of you who have read my blog or have sought orthopedic consultation in my office, I have emphasized that my recommendations are evidence based. Each patient, for whom I have completed a cellular orthopedic intervention for arthritis, has been entered into a registry or clinical outcomes data base, IRB approved. Just as I pioneered the integration of clinical care with clinical research over 37 years as a joint replacement surgeon, so too do I now partake in the growth and development of the clinical pathways for regenerative medicine.
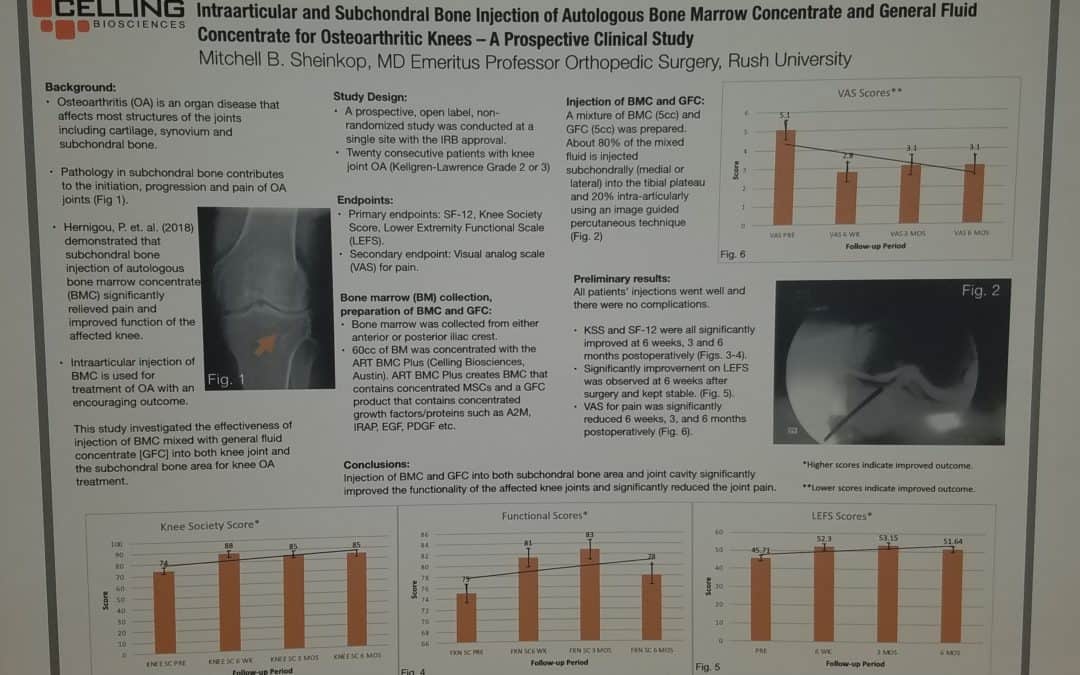
Last month, I exhibited a poster at a large regenerative medicine meeting wherein I shared my preliminary outcomes and thus educated other professionals using Intraarticular and Subchondral Bone Injection of Autologous Bone Marrow Concentrate and General Fluid Concentrate for Osteoarthritic Knees-A Prospective Clinical Study. Osteoarthritis is an organ disease that affects most structures of joints including cartilage, synovium and subchondral bone. Pathology in subchondral bone contributes to the initiation, progression and pain of Osteoarthritis. In previous European studies, the injection of autologous bone marrow concentrates into bone supporting the joint significantly relieved pain and improved function of the affected knee. The preliminary outcomes in the study that I presented via a poster exhibit, investigated the effectiveness of injections of Bone Marrow Concentrate with General Fluid Concentrate (Growth factors), into both the knee joint and the subchondral bone. The study recorded all the standard Endpoints I had previously used in joint replacement clinical outcomes trials.
Bone Marrow was collected from the pelvis and a filtration system allowed for concentration of Mesenchymal Stem Cells, Platelets, Precursor Cells and Growth factors such as A2M, IRAP, EGF, PDGF, TNF-B blocker, etc. After preparation, a mixture of Bone Marrow Concentrate and Growth factor Concentrate was injected into the bone (subchondral) and into the joint.
In the study, all patient injections went well and there were no complications. The Preliminary Results documented diminished pain and improved function. We concluded that injection of Bone Marrow Concentrate and Growth factor Concentrate into both the subchondral bone area and joint cavity significantly improved function of the affected knee joints and significantly reduced joint pain. While there are many stem cell providers to be found because of their marketing, choose the center of excellence in Cellular Orthopedics that is evidence based.
Call to schedule a scientific based consultation from an orthopedic surgeon 1 (312) 475-1893.
You may access my web site at www.SheinkopMD.com.
Tags: avascular necrosis, bone lession, bone marrow, Cartilage, cellular orthopedics, clinical study, Growth Factors, IRAP, joint pain, joint replacement, knee pain, knee replacement, meniscus tear, Osteoarthritis, platelets, PRP, regenerative medicine, sports medicine, stem cells, subchondral bone
Jun 22, 2018
My regenerative and restorative Cellular Orthopedics practice is for the most part, evidence based. By that I mean, the outcomes data collected over these past five years regarding the several thousand patients with skeletomuscular afflictions that I have treated with a selection of alternatives using a needle and not a knife is generally based on regenerative and restorative interventions. While not everyone has experienced a dramatic change in symptom relief and functional improvement, many have. The statistical outcomes evidence follows a bell shaped curve with some experiencing immediate improvement as I have in both my hips and knees, while most take several weeks or longer with a continuing improvement up to 18 months post intervention. While it is true that five percent of patients are not satisfied after several years and have gone on to a joint replacement, 95% of my patients are well satisfied and have returned to, or never quit doing what they love.
At the onset of my cellular orthopedic initiative, the interventions were solely based on Platelet Rich Plasma options and Bone Marrow Concentrate; today, our menu of services can be customized so as to meet the needs of all seeking to improve the quality of life and avoid a major surgical procedure. Not only can I concentrate PRP as needed, I can customize the concentration to meet a patient’s particular needs using hemo-analysis. Bone Marrow Concentrate rich in Adult Mesenchymal Stem cells, Platelets, Growth Factors and Precursor Cells is still the foundation of my practice, however for the past year, I am able to offer a Platelet Concentrate derived Growth Factor and Protein Solution option when indicated.
Then there are those whose co-morbidity or prescription medication dependency excludes them from the aforementioned autologous choice of options. As of this upcoming Tuesday, I have acquired an intervention technology that will help patients seeking to a void a total joint replacement who are not candidates for existing regenerative medial offerings. There are many reasons to explain a 5% failure rate including genetic cartilaginous variations, any bell shaped curve will have a small number who don’t pass the final examination. Incidentally, if and when such occurs, I offer another intervention frequently at no charge or certainly at a discounted rate.
Should you want to learn more or schedule a consultation, call
(312) 475-1896. You may visit my web site where you will find the webinar at www.Ilcellulartherapy.com.
Tags: bone marrow, cellular orthopedics, Growth Factors, Hip pain, joint pain, joint replacement, knee pain, Mesenchymal Stem Cell, Osteoarthritis, platelets
Jun 14, 2018
Over five years ago, I exchanged a scalpel for a needle and thus entered a developing discipline of cellular orthopedics. My goal was to assist patients with joint afflictions and orthopedic conditions delay, perhaps avoid a surgical procedure by capturing their body’s restorative or regenerative potential and applying evidence-based techniques.
To meet these goals, I introduced the same integration of clinical care with patient outcomes that I had pioneered over a 37-year Joint Replacement career at a major academic orthopedic center in Chicago where I retired as director of the Joint replacement Program. A data base was established and the outcomes of every patient who has undergone a Cellular Orthopedic procedure has been entered into that Data Base regulated by IRB over-site.
Now I am ready to begin sharing the outcomes we have gathered with statistically documented evidence concerning who is a candidate for Cellular Orthopedics, what is the best customized approach for a particular regenerative or restorative procedure and when to advise a patient that surgery might be a better option.
This past weekend, I had a poster exhibit on display at the TOBI meeting in Las Vegas in which I reported preliminary outcomes of a combined Intraarticular and Intraosseous (subchondroplasty) Bone Marrow Concentrate intervention for grades 2 and 3 Osteoarthritis at the knee. I am now working on four presentations as an invited guest speaker at the October meeting of Med Rebels, a well-attended regenerative medicine conference for continuing education credits concerning patient outcomes for different aspects of Cellular Orthopedic recorded in my data base.
What we have learned in these past five years plus is that everyone doesn’t respond to regenerative medicine interventions. You may best gain in-site as to why by reading a blog that I wrote exploring reasons for lack of successes: When Bone Marrow Concentrate Intervention Fails. On the other hand, in part due to the evidence I have gained as well as continuing technological advances, I have a better idea as to who is a candidate for regenerative medicine.
To learn if you are a candidate, schedule a consultation at (312) 475-1893. You may access my web site where you will find my webinar www.Ilcellulartherapy.com.
Tags: arthritis, artificial joint, blood plasma, bone marrow, bone marrow lesion, cellular orthopedics, joint pain, joint replacement, knee pain, Med Rebels, Orthopedic Surgeon, Orthopedics, Osteoarthritis, platelet, stem cells, surgery, TOBI
Apr 5, 2018
If you remember those children’s song lyrics, you will march right up the skeleton. The orthopedic message is that what’s happening in your foot and ankle will affect the well-being of your knee and hip. I was reminded of the continuum on Tuesday when a patient I had treated in November of 2017 returned for follow up this past Tuesday. Once a prominent running back at the college level, he had presented 20 years after a “high ankle sprain” with a Talar Dome Lesion at the right ankle and early onset post traumatic arthritis; in plain speak, an injury to the cartilage and underlying bone. Not only did the right ankle impairment affect his foot and ankle, he was experiencing progressive pain in his knee and hip thus altering his gait, his fitness pursuits and forcing change in his recreational profile. Running was no longer possible nor was snowboarding.
Increasingly, these Talar Dome lesions or osteochondral injuries are being diagnosed long after what was thought to have been a sprained ankle. In the case of my patient, last November, I performed a minimally invasive procedure wherein bone marrow was aspirated from his pelvis, concentrated, processed, and injected into both the ankle joint and bone marrow defect of the talus under fluoroscopic guidance. Osteochondral injuries and bone marrow lesions are a continuum of small posttraumatic defects that pathologists have shown represent a failed healing response. Most readily diagnosed on an MRI, with time, a rim of sclerosis may develop so the abnormality may lend itself to diagnosis with an X-ray. This type of defect is not limited to the ankle and may be found throughout the extremities and pelvis. They may be found in any joint region that sees weight bearing or repetitive stress though; most commonly, they are associated with trauma as was the case, though long removed in my patient.
In the case of this vignette, on Tuesday I had determined that ankle and subtalar joint motions had become symmetrical. He no longer complained of pain; equally important, the bony defect and joint changes could no longer be seen on X-ray. In short, he had healed. In the past six months, I have followed two other equally rewarding Bone Marrow (stem cell/growth factor/platelet) intervention outcomes at the talus and more than six around the knee.
If you are experiencing joint pain and altered function without an explanation or in spite of a course of “conservative” treatment, it may be time to learn more about how Bone Marrow Concentrate, that is stem cells, platelets and growth factors, may relieve bone and joint pain, restore function and help you postpone, perhaps even avoid a major surgical procedure.
Call 312 475 1896 to schedule a consultation or visit my web site and watch the webinar at www.ilcellulartherapy.com
Tags: ankle pain, bone lesion, bone marrow, Cartilage, joint pain, Mesenchymal Stem Cell, Osteoarthritis, osteochondral defect, osteochondral injurie, Osteochondritis Dissecans, Subchondroplasty, Talar Dome lesions