
Dec 5, 2018
As interest in biologic therapies for arthritis-a needle, not a knife-continues to expand; patients increasingly are turning to the ads in newspapers or searching the Internet to gather information on this topic. While there is still a lack of scientific consensus on the use of biologics, it is most important for those seeking information not to be misled. My own analysis of resources for patients seeking on line information about biologic therapies for arthritis is that the overall quality is very poor and anything but scientific. Even worse, is a seminar, neither a reliable or credible source of scientific evidence.
Biologic therapies consist of stem cells, platelet rich plasma product and bone marrow aspirate concentrate. New research, I co-authored and that was published last month in The American Journal of Orthopedics: Safety and Efficacy of Micro-Fractured Adipose Tissue for Knee Arthritis, is indicative of the ever-evolving nature of Regenerative Medicine. Biologic therapies and their use in arthritis or musculoskeletal injury in general are an area of vast research and interest within the medical field. Understanding the information online and the misinformation provided at seminars pertaining to biologics allows me to tailor my conversation and address commonly found inaccuracies.
The use of Biologic Therapies is expected to significantly increase in the coming years as our knowledge advances on the use of such. That initiative will be led by well informed, well-educated Board Certified, and Fellowship trained specialists. Unfortunately owing to the relative lack of oversite at present, every type of charlatan, parasite and camp follower can buy an ad for a seminar or produce a web site on the internet. How then should a patient with pain and limited function from arthritis seek to postpone or avoid surgery without becoming a victim of the cord blood or amniotic fluid hoax?
- Your physician must complete a comprehensive medical history, physical examination and review of diagnostic studies.
- Explain the disease process and grade of progression,
- Discuss possible treatment options,
- Present a balanced assessment of the current scientific evidence.
Woe, while writing this Blog, I was just notified about acceptance of yet another scientific article by a peer reviewed medical journal in which I am the senior author: A Specific Protocol of Autologous Bone Marrow Concentrate and Platelet Products Versus Exercise Therapy for Symptomatic Knee Osteoarthritis; a Randomized Control Trial with 2 Year Follow-up.
Hopefully some time soon, a Biologic Arthroplasty will be possible; but until then, a Total Joint Replacement is still a necessary option for those not meeting specified inclusion criteria for biologics. To see what treatments may be possible for your arthritic generated pain call (312) 475-1893 to schedule a consultation. Visit my website www.SheinkopMD.com for additional information.
Tags: Adult Mesenchymal Stem Cells, amniotic fluid, ankle pain, arthritic pain, autologous bone marrow concentrate, biologic, biologics, cellular orthopedics, Cord blood, Hip pain, injury, joint pain, knee pain, lipogems, Osteoarthritis, PRP, regenerative medicine, rupture, shoulder pain, sports injury, stem cell, tear, tendinitis

Nov 29, 2018
My Blog has frequently addressed the false ads claiming Amniotic Fluid, Chord Blood, Wharton’s Jelly and the like contain living stem cells emphasizing that the processes of preservation and sterilization followed by freezing kills off any living cells. Sylvia Perez first addressed the issue on Fox News’ Conversation in Health, January 29, 2018 and Pam Zekman posted her investigative report on WBBM-TV, the week before Thanksgiving. Yet patients continue falling for the hoax.
In contrast, let’s address the positive, cellular orthopedics; the ongoing practice of evidence- based medicine. Below are two statistically significant scientific studies that play a role in helping determine the best possible outcomes to a regenerative intervention
November 21, 2018
Safety and Efficacy of Micro-Fractured Adipose Tissue for Knee Osteoarthritis
New research published by TOBI Faculty suggests autologous, micro-fractured, minimally manipulated adipose tissue may represent a nonsurgical treatment option for knee osteoarthritis patients seeking alternatives to total knee replacement.
Congratulations Jay Panchal, MD, Gerard Malanga, MD, Mitchell Sheinkop, MD on this new publication in The American Journal of Orthopedics.
Safety and Efficacy of Percutaneous Injection of Lipogems Micro-Fractured Adipose Tissue for Osteoarthritic Knees
To download or read the publication: https://www.amjorthopedics.com/article/safety-and-efficacy-percutaneous-injection-lipogems-micro-fractured-adipose-tissue
Treatment of Knee Osteoarthritis with Autologous Bone Marrow Concentrate and Cytokine Concentrate – A Prospective Clinical Case Series Study
Abstract submitted to the Orthopedic Research Society Annual Meeting, 2019
Mitchell B. Sheinkop1 , Marry Langhenry2 , Jizong Gao3 1. Orthopedic Surgery, Rush University, Chicago, IL.2. Cellular Orthopedics, Chicago, IL 3. Celling Biosciences, Austin, Texas.
INTRODUCTION: Osteoarthritis (OA) is an organ disease that affects most structures of the joints including cartilage, synovium and subchondral bone. The pathophysiology of knee osteoarthritis can be broken down into pathoanatomy, cell biology, and genetics. Although fibrillation of articular cartilage is regarded as the primary changes and potential cause of clinical symptoms, the synovium and capsule undergo progressively inflammatory changes and secrete proteolytic enzymes that may contribute to the progression of OA. Meanwhile, the subchondral bone tissue develops lytic lesions with edema, sclerosis, and cyst formation. Therefore, it has been recommended that the treatment of OA should be a comprehensive approach to create a homeostatic environment to facilitate the OA treatment with a long-lasting outcome. Bone marrow contains mesenchymal stem cells (MSCs). Different cytokines such as alpha 2-macroglobulin (A2M) (Wang et al) and growth factors have been identified in the blood and bone marrow aspirate. Either bone marrow concentrate (BMC) or MSCs have been injected into the knee joint to treat OA with promising clinical outcomes. Hernigou et al reported that injection of BMC into the subchondral bone area was able to delay or eliminate the need for total knee arthroplasty (TKA) and clinical outcome was comparable to TKA in the contralateral knee. Cytokines and growth factors in the blood or bone marrow aspirate were concentrated by filtering method to prepare autologous therapeutic biologics. In the current study, a consecutive series of patients with moderate to severe OA were treated by intra-articular and intra-subchondral bone injection of BMC and autologous concentrated cytokines/growth factors. The quantity of representative cytokines and growth factors in the concentrate were also measured. Patients were evaluated for the improvement of systems and knee functions by following up to 6 months after injection. METHODS: This prospective case series study was approved by the Institutional Review Board.
To learn more or to schedule an evidence-based consultation call (312) 475-1893
You may visit my web site and read my blogs at www.sheinkopmd.com
Regenerative Medicine is an option for those with arthritis but don’t be fleeced by the hucksters and camp followers.
Tags: autologous bone marrow concentrate, biologics, BMC, cellular orthopedics, cytokine concentrate, Growth Factors, knee pain, lipogems, Micro-Fractured Adipose, MSC, OA, Orthopedic Surgeon, Osteoarthritis, PRP, regenerative medicine, stem cells, suchondral, TOBI
Oct 18, 2018
We are speaking of stem cell therapy integrated with clinical research, and the resultant evidence-based stem cell intervention. Osteoarthritis is becoming more prevalent as I am seeing younger patients with arthritis as a consequence of sporting injuries such as ACL tears. The baby boomer population is experiencing accelerated onset of arthritis; their joints are prematurely aging in large numbers. At the same time, the master population is aging and living longer. As a result, I continually research biologic interventions to best address the ever-increasing number of those effected.
Why should a patient choose an orthopedic surgeon to manage their Osteoarthritic related symptoms and functional impairment? Our world is evidence based.
Study Observes Better Outcomes for OA Patients Treated by an Orthopaedic Specialist
In a retrospective study published online in BMC Musculoskeletal Disorders, shoulder osteoarthritis (OA) patients received faster and more invasive treatment when they received a new diagnosis from an orthopaedic specialist (OS) versus a nonorthopaedic physician (NOP). Patients with shoulder OA (n = 572) received care from either an OS (n = 474) or NOP (n = 98) on the date of their index shoulder visit. OS patients received their first treatment significantly quicker than the NOP cohort (16.3 days versus 32.3 days, respectively). The OS group also had higher rates of operative treatment within one year following their initial visit.
Study: Patients Report Similar Improvements for Nonobstructive Meniscal Tear with PT and Early Surgery
Physical therapy (PT) may not be inferior to early operative treatment of arthroscopic partial meniscectomy (APM) for improving knee functionality in patients with nonobstructive meniscal tears, according to a study published online inJAMA. The randomized clinical trial included 321 patients with nonobstructive meniscal tears aged 45 to 70 years who were treated at nine hospitals in the Netherlands between July 17, 2013, and Nov. 4, 2015. Patients were treated with APM (n = 159) or a predefined PT protocol (n = 162) that included 16 exercise therapy sessions over eight weeks. PT sessions focused on coordination and closed kinetic chain strength exercises. At 24-month follow-up, knee functionality in the PT group improved by 20.4 points compared to 26.2 points in the APM group. The difference did not exceed the noninferiority margin.
In order to maximize the benefits, Orthobiologics, that is stem cell therapy must be integrated with clinical research, and the resultant evidence-based stem cell intervention followed long term. In my practice, I am researching biologic interventions to address the ever-increasing number of those effected, not one and done. To learn more or schedule a consultation, Call (312)475-1893. You may visit my web site and read my blogs at www.sheinkopmd.com
Tags: ACL tear, arthritis, Cartilage, cellular orthopedic, joint pain, joint replacement, knee pain, MCL tear, meniscus tear, menisectomy, orthobiologics, orthopedic surgen, Osteoarthritis, Physical Therapy, PRP, regenerative medicine, stem cell

Oct 5, 2018
After reviewing a CT scan of the right knee where a Total Knee Replacement had been done provided by a patient who sought my opinion for stem cell treatment of her arthritic left knee, I called her to discuss the possible reasons that the right Total Knee Replacement that she had undergone over ten years ago was never satisfactory. At the time of the right TKR for arthritis, she had elected for what seemed at the time as a logical intervention for a painful, arthritic, right knee. The outcome was at first complicated by a lot of postoperative swelling and pain; at one-year post-operative, the patient had never been pain-free nor had she ever regained her preoperative range of motion and that adverse outcome has persisted for over ten years. Fast forward a decade and the right knee has continued to be a source of pain and limited motion; so much so that the patient decided to seek consultation for a Stem Cell treatment for her now arthritic left knee.
Her first question was basically “does stem cell therapy for knees work?”. Our data collected on patients treated in this office over the past six years, since I started my practice, is compatible with an 85% patient satisfaction rate. We have not recorded one complication. To be forthright, not every patient has a perfect result; but the vast majority experience marked reduction in pain, increased motion and a significant improvement in functional capacity. Unlike a failed outcome of a Total Knee Replacement, our stem cell injections may be repeated at anytime if the benefits of the initial intervention do not last.
When it comes to the cost of a stem cell intervention, while the Total Joint Replacement is more often than not covered by some type of insurance, our fee schedule is in keeping in line with the deductible a patient has to pay out of pocket for the major surgery. If you do the math and additionally compare the risks and benefits of a stem cell intervention with a total knee replacement, you will note:
- Remote to little risk of complication with a stem cell procedure
- Comparable cost comparing my charges for a stem cell intervention with the inherent deductible obligation for a Total Joint Replacement
- Rapid recovery with a stem cell intervention versus the risks of an adverse outcome as experienced by the patient seeking consultation for stem cells
To seek consultation call (312) 475-1893. You may visit my website at WWW.sheinkopmd.com
Tags: cellular orthopedics, ct scan, joint health, joint replacement, knee pain, knee replacement, Osteoarthritis, regenerative medicine, stem cell treatment, TKA
Jul 19, 2018
The argument frequently advanced by orthopedic surgeons in response to a patient’s inquiry concerning stem cells for arthritis is that it is too early, there is not enough research, It is better to have a major surgical procedure. For those of you who have read my blog or have sought orthopedic consultation in my office, I have emphasized that my recommendations are evidence based. Each patient, for whom I have completed a cellular orthopedic intervention for arthritis, has been entered into a registry or clinical outcomes data base, IRB approved. Just as I pioneered the integration of clinical care with clinical research over 37 years as a joint replacement surgeon, so too do I now partake in the growth and development of the clinical pathways for regenerative medicine.
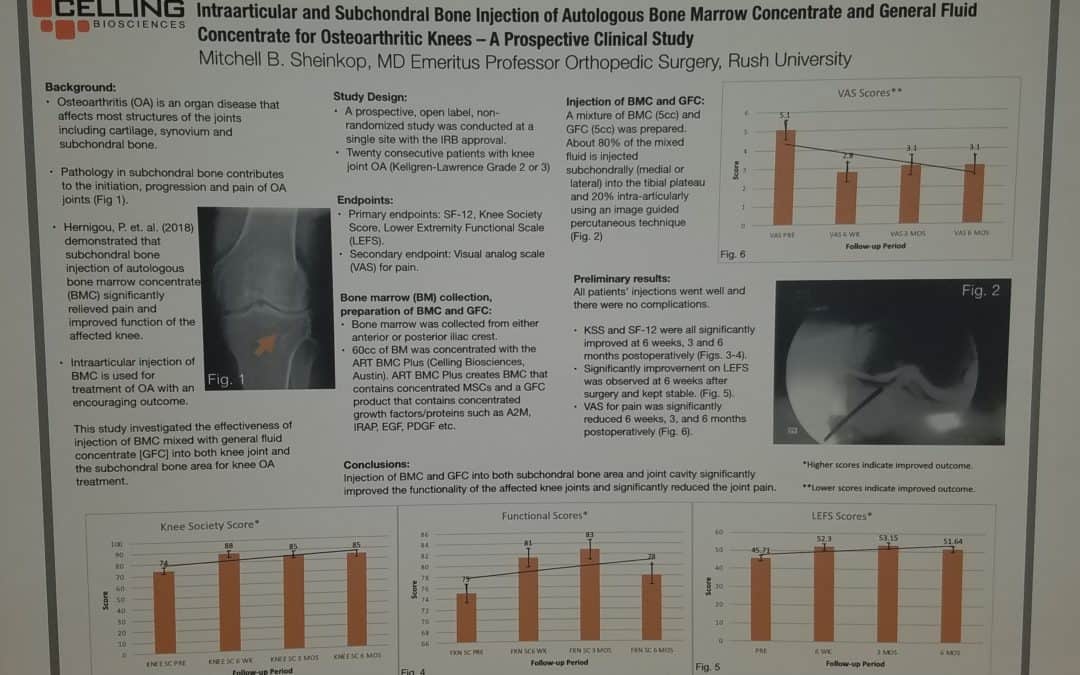
Last month, I exhibited a poster at a large regenerative medicine meeting wherein I shared my preliminary outcomes and thus educated other professionals using Intraarticular and Subchondral Bone Injection of Autologous Bone Marrow Concentrate and General Fluid Concentrate for Osteoarthritic Knees-A Prospective Clinical Study. Osteoarthritis is an organ disease that affects most structures of joints including cartilage, synovium and subchondral bone. Pathology in subchondral bone contributes to the initiation, progression and pain of Osteoarthritis. In previous European studies, the injection of autologous bone marrow concentrates into bone supporting the joint significantly relieved pain and improved function of the affected knee. The preliminary outcomes in the study that I presented via a poster exhibit, investigated the effectiveness of injections of Bone Marrow Concentrate with General Fluid Concentrate (Growth factors), into both the knee joint and the subchondral bone. The study recorded all the standard Endpoints I had previously used in joint replacement clinical outcomes trials.
Bone Marrow was collected from the pelvis and a filtration system allowed for concentration of Mesenchymal Stem Cells, Platelets, Precursor Cells and Growth factors such as A2M, IRAP, EGF, PDGF, TNF-B blocker, etc. After preparation, a mixture of Bone Marrow Concentrate and Growth factor Concentrate was injected into the bone (subchondral) and into the joint.
In the study, all patient injections went well and there were no complications. The Preliminary Results documented diminished pain and improved function. We concluded that injection of Bone Marrow Concentrate and Growth factor Concentrate into both the subchondral bone area and joint cavity significantly improved function of the affected knee joints and significantly reduced joint pain. While there are many stem cell providers to be found because of their marketing, choose the center of excellence in Cellular Orthopedics that is evidence based.
Call to schedule a scientific based consultation from an orthopedic surgeon 1 (312) 475-1893.
You may access my web site at www.SheinkopMD.com.
Tags: avascular necrosis, bone lession, bone marrow, Cartilage, cellular orthopedics, clinical study, Growth Factors, IRAP, joint pain, joint replacement, knee pain, knee replacement, meniscus tear, Osteoarthritis, platelets, PRP, regenerative medicine, sports medicine, stem cells, subchondral bone