
Jul 26, 2018
Hip osteoarthritis (OA) exerts a significant burden on society, affecting 3% of Americans aged >30 years. Recent advances in the understanding of the pathoanatomy and pathomechanics of the hip have led to treatment options for young adults with hip pain. Femoroacetabular impingement, specifically cam-type femoroacetabular impingement, hip dysplasia, and the sequelae of pediatric hip disease can predispose the hip to early OA. However, many patients with abnormal anatomic findings do not develop early OA, suggesting that there exist other patient characteristics that are protective despite abnormal bony anatomy. Outcome studies show that arthroscopic and open hip procedures improve pain and function in patients with symptomatic hips. However, there is currently limited evidence that these procedures extend the life of the patient’s natural hip. Additional studies are needed to determine protective or adaptive factors in patients with abnormal anatomy who do not develop early OA and to determine whether joint preserving hip surgery extends the life of the native hip joint.
Review Article:Natural History of Structural Hip Abnormalities and the Potential for Hip Preservation
James D. Wylie, Christopher L. Peters, Stephen Kenji Aoki
What makes the article so interesting to me is first, I played a role in training one of the authors in my earlier academic career. More important is the role I am now playing in helping to preserve the life of the hip joint with a needle instead of a knife and extending the life of the “native hip joint”. The latter is done via Cellular Orthopedics. By introducing Stem Cells, Platelets, Precursor Cells, and Growth Factors, I am now able to address arthritis at a Bio-Immune level, possibly regenerate cartilage, potentially influence healing of the torn acetabular labrum, certainly reverse the secondary inflammation and thereby diminish pain and improve function in the abnormal hip joint.
It takes an evaluation in my office including the history, a physical examination and my review of your hip images after which I am able to customize the Cellular Orthopedic intervention that will help with joint preservation and potentially, joint regeneration. Our Outcomes studies continue and it is the result of ongoing data collection that allows me to extend the life of your native hip. Call (312) 475 1893 to schedule a consultation. You may visit my web site at www.sheinkopmd.com
Tags: cellular orthopedics, Dysplasia, Hip osteoarthritis, Hip pain, hip surgery, platelets, stem cells, torn labrum
Jul 19, 2018
The argument frequently advanced by orthopedic surgeons in response to a patient’s inquiry concerning stem cells for arthritis is that it is too early, there is not enough research, It is better to have a major surgical procedure. For those of you who have read my blog or have sought orthopedic consultation in my office, I have emphasized that my recommendations are evidence based. Each patient, for whom I have completed a cellular orthopedic intervention for arthritis, has been entered into a registry or clinical outcomes data base, IRB approved. Just as I pioneered the integration of clinical care with clinical research over 37 years as a joint replacement surgeon, so too do I now partake in the growth and development of the clinical pathways for regenerative medicine.
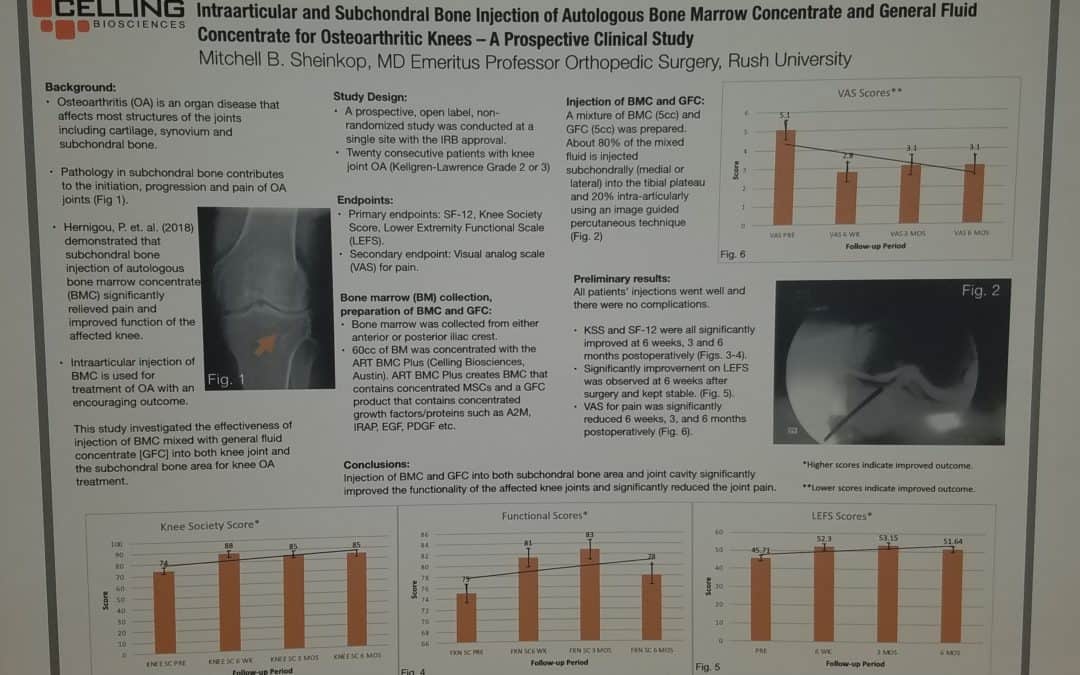
Last month, I exhibited a poster at a large regenerative medicine meeting wherein I shared my preliminary outcomes and thus educated other professionals using Intraarticular and Subchondral Bone Injection of Autologous Bone Marrow Concentrate and General Fluid Concentrate for Osteoarthritic Knees-A Prospective Clinical Study. Osteoarthritis is an organ disease that affects most structures of joints including cartilage, synovium and subchondral bone. Pathology in subchondral bone contributes to the initiation, progression and pain of Osteoarthritis. In previous European studies, the injection of autologous bone marrow concentrates into bone supporting the joint significantly relieved pain and improved function of the affected knee. The preliminary outcomes in the study that I presented via a poster exhibit, investigated the effectiveness of injections of Bone Marrow Concentrate with General Fluid Concentrate (Growth factors), into both the knee joint and the subchondral bone. The study recorded all the standard Endpoints I had previously used in joint replacement clinical outcomes trials.
Bone Marrow was collected from the pelvis and a filtration system allowed for concentration of Mesenchymal Stem Cells, Platelets, Precursor Cells and Growth factors such as A2M, IRAP, EGF, PDGF, TNF-B blocker, etc. After preparation, a mixture of Bone Marrow Concentrate and Growth factor Concentrate was injected into the bone (subchondral) and into the joint.
In the study, all patient injections went well and there were no complications. The Preliminary Results documented diminished pain and improved function. We concluded that injection of Bone Marrow Concentrate and Growth factor Concentrate into both the subchondral bone area and joint cavity significantly improved function of the affected knee joints and significantly reduced joint pain. While there are many stem cell providers to be found because of their marketing, choose the center of excellence in Cellular Orthopedics that is evidence based.
Call to schedule a scientific based consultation from an orthopedic surgeon 1 (312) 475-1893.
You may access my web site at www.SheinkopMD.com.
Tags: avascular necrosis, bone lession, bone marrow, Cartilage, cellular orthopedics, clinical study, Growth Factors, IRAP, joint pain, joint replacement, knee pain, knee replacement, meniscus tear, Osteoarthritis, platelets, PRP, regenerative medicine, sports medicine, stem cells, subchondral bone
Jul 12, 2018
Just as I cringe when a new patient announces that they have “bone on bone”, so too do I squirm when I am told by a patient “I have a torn” at times meniscus or cartilage; others, a torn rotator cuff; and then again, a torn labrum. Attention please, your X-ray or MRI image is not causing pain, the inflammation in or around your joint is the pain generator. 95% of the population over age 45 will have an abnormality interpreted by the radiologist on the report their MRI, be it of the shoulder, hip or knee. Cartilage and meniscal changes at the knee, labral tears at the hip or shoulder, and rotator cuff abnormalities are part of the attritional process; alternatively, these changes are commonly over diagnosed.
Last week, a 70-year-old woman called to schedule an appointment and indicated that she had a torn acetabular(hip) labrum diagnosed on a recent MRI. I responded, “your pain generator is arthritis unless you are a hockey goalie”. I was being a bit facetious but at the same time truthful. My 37-year experience as a reconstructive orthopedic surgeon specializing in hip and knee replacement really prepared me for this life after surgery; namely, a cellular orthopedic interventionalist.
It takes a history and hands on physical examination prior to review of images to determine what is causing a painful musculoskeletal condition. The common denominator is inflammation, not a computer image. In the case of arthritis, unless the cartilage (meniscus), labrum or rotator cuff alteration is generating mechanical problems such as weakness, locking, “clunking” or giving way, we frequently need not address the former with a maximally invasive surgical procedure; a needle will suffice and deliver the platelets, Mesenchymal Stem Cells, Growth Factors and precursor cells required to address pain, improve function, increase motion, stop progression of arthritis and restore, at times regenerate the joint.
Cellular Orthopedics encompasses a full joint Preservation, Restoration and Regenerative scope of options. The notion introduced by a print media ad, that it is “one and done”, won’t help you postpone, perhaps avoid a joint replacement. In my practice, we monitor progress and intervene when necessary at five months or five years if indicated.
To learn more, visit my web site at www.SheinkopMD.com or call and schedule a consultation at (312) 475-1893
Tags: arthritis, bone lesion, Bone Marrow Concentrate, cellular orthopedics, hip pian, joint pain, joint replace, knee pain, meniscus, Osteoarthritis, PRP, Rotator cuff, stem cells, stiffness, torn labrum
Jun 22, 2018
My regenerative and restorative Cellular Orthopedics practice is for the most part, evidence based. By that I mean, the outcomes data collected over these past five years regarding the several thousand patients with skeletomuscular afflictions that I have treated with a selection of alternatives using a needle and not a knife is generally based on regenerative and restorative interventions. While not everyone has experienced a dramatic change in symptom relief and functional improvement, many have. The statistical outcomes evidence follows a bell shaped curve with some experiencing immediate improvement as I have in both my hips and knees, while most take several weeks or longer with a continuing improvement up to 18 months post intervention. While it is true that five percent of patients are not satisfied after several years and have gone on to a joint replacement, 95% of my patients are well satisfied and have returned to, or never quit doing what they love.
At the onset of my cellular orthopedic initiative, the interventions were solely based on Platelet Rich Plasma options and Bone Marrow Concentrate; today, our menu of services can be customized so as to meet the needs of all seeking to improve the quality of life and avoid a major surgical procedure. Not only can I concentrate PRP as needed, I can customize the concentration to meet a patient’s particular needs using hemo-analysis. Bone Marrow Concentrate rich in Adult Mesenchymal Stem cells, Platelets, Growth Factors and Precursor Cells is still the foundation of my practice, however for the past year, I am able to offer a Platelet Concentrate derived Growth Factor and Protein Solution option when indicated.
Then there are those whose co-morbidity or prescription medication dependency excludes them from the aforementioned autologous choice of options. As of this upcoming Tuesday, I have acquired an intervention technology that will help patients seeking to a void a total joint replacement who are not candidates for existing regenerative medial offerings. There are many reasons to explain a 5% failure rate including genetic cartilaginous variations, any bell shaped curve will have a small number who don’t pass the final examination. Incidentally, if and when such occurs, I offer another intervention frequently at no charge or certainly at a discounted rate.
Should you want to learn more or schedule a consultation, call
(312) 475-1896. You may visit my web site where you will find the webinar at www.Ilcellulartherapy.com.
Tags: bone marrow, cellular orthopedics, Growth Factors, Hip pain, joint pain, joint replacement, knee pain, Mesenchymal Stem Cell, Osteoarthritis, platelets
Jun 14, 2018
Over five years ago, I exchanged a scalpel for a needle and thus entered a developing discipline of cellular orthopedics. My goal was to assist patients with joint afflictions and orthopedic conditions delay, perhaps avoid a surgical procedure by capturing their body’s restorative or regenerative potential and applying evidence-based techniques.
To meet these goals, I introduced the same integration of clinical care with patient outcomes that I had pioneered over a 37-year Joint Replacement career at a major academic orthopedic center in Chicago where I retired as director of the Joint replacement Program. A data base was established and the outcomes of every patient who has undergone a Cellular Orthopedic procedure has been entered into that Data Base regulated by IRB over-site.
Now I am ready to begin sharing the outcomes we have gathered with statistically documented evidence concerning who is a candidate for Cellular Orthopedics, what is the best customized approach for a particular regenerative or restorative procedure and when to advise a patient that surgery might be a better option.
This past weekend, I had a poster exhibit on display at the TOBI meeting in Las Vegas in which I reported preliminary outcomes of a combined Intraarticular and Intraosseous (subchondroplasty) Bone Marrow Concentrate intervention for grades 2 and 3 Osteoarthritis at the knee. I am now working on four presentations as an invited guest speaker at the October meeting of Med Rebels, a well-attended regenerative medicine conference for continuing education credits concerning patient outcomes for different aspects of Cellular Orthopedic recorded in my data base.
What we have learned in these past five years plus is that everyone doesn’t respond to regenerative medicine interventions. You may best gain in-site as to why by reading a blog that I wrote exploring reasons for lack of successes: When Bone Marrow Concentrate Intervention Fails. On the other hand, in part due to the evidence I have gained as well as continuing technological advances, I have a better idea as to who is a candidate for regenerative medicine.
To learn if you are a candidate, schedule a consultation at (312) 475-1893. You may access my web site where you will find my webinar www.Ilcellulartherapy.com.
Tags: arthritis, artificial joint, blood plasma, bone marrow, bone marrow lesion, cellular orthopedics, joint pain, joint replacement, knee pain, Med Rebels, Orthopedic Surgeon, Orthopedics, Osteoarthritis, platelet, stem cells, surgery, TOBI