May 31, 2018
It is the most banal, recurring, boring, ordinary and meaningless phrase that my assistant and I have to listen to on the phone or at every office setting. Osteoarthritis is a disease that affects almost all persons to some extent as they age. It may affect one joint, some joints or many joints. The causes may include genetic predisposition, trauma, or any of varying diseases at different ages. No matter the causation be the arthritis primary or secondary, the presentation is progressive pain and decreasing function. The X-ray is diagnostic in most cases: loss of cartilage joint space, subchondral sclerosis and osteophyte formation. The pain generator is inflammation and not bone on bone. Images help with diagnosis; but the degree of arthritic change on X-ray does not necessarily correlate with the severity of the symptoms or the functional impairment.
A normal joint has a bony support, a cartilage interface, a synovial lining, a capsular envelope, stabilizing ligaments and surrounding muscle. All these anatomic structures are affected by the inflammation associated with degenerative changes on a bio-immune basis. When a physician undertakes the care of an arthritic joint, the management is based on addressing the inflammatory pain generators and not until the subchondral bone is severely altered and the cartilage gliding surface has been severely destroyed is a joint replacement indicated (Grade 4 OA). Until that time the classic approach has been weight loss, anti-inflammatories either by mouth or via injection, bracing, strength training, range of motion therapy; that is, until the new world of cellular orthopedics came into being.
My initial approach in my practice is to address pain and altered function from inflammation of osteoarthritis, not “bone on bone”. By a combination and concentration of platelets and growth factors, I now have the ability to reverse the pain generating arthritic inflammation and alter the bio-immune basis for degeneration of the joint; this is called joint preservation. On the other hand, my initiative for joint regeneration is based on autologous bone marrow concentrate; the latter containing in addition to platelets and growth factors, adult mesenchymal stem cells, precursor cells, hemopoietic stem cells and more. The attempts at joint regeneration are directed both to the joint itself by intraarticular injection and subchondral injection; the latter to help repair the supporting bone.
There is a lot to process here so let me address your needs best and answer your questions following an office assessment and a review of images. Call (312) 475-1893 to schedule a consultation. You may learn more on my website www.Ilcellulartherapy.com where you will find our webinar
Tags: arthritis, Bone Marrow Concentrate, bone on bone, Cartilage, Hip pain, joint pain, knee pain, Mesenchymal Stem Cell, Osteoarthritis, PRP, Regenerative Pain Center
May 14, 2018
“Mitch, not sure if you heard, but the FDA via the DOJ has requested injunctions against the mothership clinics of Berman and Lander, as well as the US Stem Cell clinic run by Comella. We can hope that criminal indictments might follow, since they certainly are some of the most flagrant violators of the law in recent med I can think of. The SCIA group can’t be too far behind. It seems that advertising all kinds of cures for everything that ails the patient makes you a higher priority target.” (Personal communication)
I am dedicated to providing patients with the best possible care in regenerative medicine and am pleased to announce that I have adopted a technology platform developed by Greyledge Technologies (Vail, CO). Their technology to generate platelet-rich plasma (PRP) and bone marrow-derived cell concentrate (BMC) is derived from successfully operating a laboratory that is registered with the FDA (listed as a “component preparation and collection facility”, FEI 3008724474), which has cleared two audits with no issues. Based on their platform, I offer my patients customized therapy, since each preparation is analyzed for platelets, red blood cells and white blood cells (among 23 parameters), which I review prior to treatment. This knowledge permits me to make adjustments based on my more than 40 years of experience in orthopedic surgical and now cellular orthopedic practice. No other system or technology gives me this kind of capability to personalize your treatment.
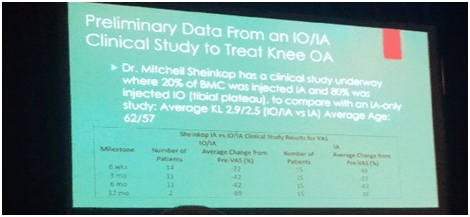
As a result of the technology I have adopted, my office has been able to create a scientific outcomes data base using the same parameters in cellular orthopedics as when I was the director at one of the five largest joint replacement programs in the country. At that time, I pioneered the integration of patient are with research and education. The latter allowed me to rise to the position of full professor; having publish over 75 scientific articles in the field of hip and knee joint replacement. I am happy to update you with the fact that I am at it again. On June 10, my paper concerning the preliminary outcomes of combined intraarticular and intraosseous stem cell intervention for knee arthritis will be presented in Las Vegas at of The Orthopedic and Biologic Institute (TOBI) annual meeting. The manuscript concerning Autologous Bone Marrow Concentrate and Platelet Product for Symptomatic Knee Arthritis: A Randomized Controlled Trial, Minimum 2 Year Follow-Up was submitted to a major orthopedic journal and is one of three papers I have been invited to deliver from the scientific podium of The Medrebels, October 26 to 28 meeting in Austin, Texas.
If you want to avail yourself of the best opportunity to postpone, perhaps avoid a joint replacement for arthritis while enjoying pain relief and restoration of an active life style, chose science over advertised anecdote. Call (312) 475-1893 to schedule an appointment. You may access my website and watch the webinar at www.Ilcellulartherapy.com.
Tags: APGC injection, arthritis, BMC injection, Bone Marrow Concentrate, bone on bone, Greyledge, Growth Factor Concentrate, Hip pain, intraarticular, intraosseous, joint pain, knee pain, Medrebels, Osteoarthritis, PRP, stem cell intervention, TOBI

Apr 16, 2018
My team dedicates an inordinate amount of time answering questions and attempting to clarify the misunderstanding of patients when it comes to Platelet Rich Plasma; actually, the entire subspecialty of “Stem Cell Therapy” but let’s start with PRP. As an orthopedic surgeon who introduced Cellular Orthopedics to the Midwest five years ago, I am in a unique position to help define the problem. Does PRP have a role in treating a painful or injured part of the musculoskeletal system? In an attempt to help clarify misconceptions and better define the term Platelet Rich Plasma, I sat down and wrote this Blog.
Platelets circulating in the blood play a fundamental role in blood clotting and are a natural source of growth factors. Platelet rich plasma (PRP), also termed autologous platelet gel, plasma rich in growth factors (PRGF), platelet concentrate (PC), is essentially an increased concentration of (autologous) your platelets suspended in a small amount of plasma after centrifugation. Although it is not exactly clear how PRP works, laboratory studies have shown that the increased concentration of growth factors in PRP can potentially speed up the healing process.
The amount of PRP necessary to achieve the intended biologic effects still remains unclear.; but we know PRP contains growth factors in high concentrations. Precise predictions of growth factor levels based on the platelet counts of whole blood or PRP are limited. In our office, we use a hemocytometer to count platelets and the different white blood cells contained in the preparation. Knowing there are different sources for growth factors (platelets, leukocytes, plasma), we assume the higher number of platelets and leukocytes counted in the hemocytometer, the higher the concentration of growth factors in the preparation. Treatments using these autologous platelet growth factors are an important reason to improve methods for isolating platelet-rich plasma (PRP) and that is why I am involved in an initiative to correlate counts with clinical outcomes.
PRP proponents assert that concentrated Platelet Rich Plasma fails to successfully treat symptoms in some cases because of differences in PRP formulation. There is no standardization thus leading to variables, such as PRP preparation methods, the amount of PRP injected, and the frequency of injections. These inconsistencies result in issues raised by patients: “PRP didn’t work for me” and “I had 15 PRP injections to my knee and I still have pain”. In addition to studying the numbers and monitoring results, I am involved with initiatives to filter and concentrate the growth factors in PRP so as to improve outcomes as well.
1)Platelet Rich Plasma
2)Concentrated Platelet Rich Plasma
3)Concentrated Stem Cell Plasma
4)Autologous Platelet and Growth Factor Concentrate
When you call (312- 475- 1893) to schedule a consultation or watch my webinar at www.Ilcelulartherapy.com, you will avail yourself of the aforementioned Platelet Rich Plasma treatment options in addition to our entire Cellular Orthopedic menu of regenerative care.
Tags: autologous injection, autologous platelet and growth factor concentrate, hemocytometer, injection, leukocytes, Platelet Rich Plasma, PRGF, PRP, Stem Cell Plasma
Feb 16, 2018
I am sitting at my computer this morning writing the weekly Blog posting and not attending the IOF meeting taking place today in Broomfield, Colorado; yet I am reporting about the meeting. Instead of attending, I am preparing for a week-long ski adventure with my family next week in Vail, Colorado while trying to catch up in my practice. How is it than possible that I know what is taking place at the meeting? Listed below are five of the 10 ongoing or completed cellular orthopedic clinical trials in which I am a principal investigator or co-researcher. The preliminary and final data resulting from these clinical research initiatives is the outcomes foundation for what is being presented at the IOF podium today and tomorrow.
1) Stem Cell Counts and the Outcome of Bone Marrow Concentrate intra-articular and intra-osseous (subchondroplasty) interventions at the knee for grades 2 and 3 OA. (supported in part by Celling). Ongoing
2) Outcomes of Bone Marrow Concentrate (stem cell, platelet and growth factor) Intervention at the Knee for Grades 2 and 3 OA in 50 patients at 2 to 4 years. (supported in part by Regenexx)
3) Outcomes of Intra-articular Bone Marrow Concentrate versus those of combined Intraarticular and Intraosseous interventions for grades 2 and 3 OA at the knee at one year. (self-funded). Ongoing
4) How does the PRP and Mononucleated cell count affect the outcome of a BMC intervention for grades 2 and 3 Knee OA? (a joint project with Greyledge) Ongoing
5) Safety and Efficacy of Percutaneous Injection of Micro-Fractured Adipose Tissue for grade 4 Osteoarthritic Knees, minimum follow-up of 18 months in 30 patients (supported in part by Lipogems)
I had to prioritize; and since most of the arthritis data being presented is all or in part mine, I already know the subject matter. By staying home, I also found the opportunity to browse “stem cell” websites as suggested by ads in today’s newspapers or introduced by email blasts this week. Wow, a patient acting more like a consumer is really at risk for succumbing to Regenerative Medicine “false news”.
If you want to learn more about the difference between the stem cell purveyors and a legitimate, FDA compliant, evidence based, cellular orthopedics initiative, call to schedule a consultation or to get a second opinion.
You may schedule a visit at (312) 475-1893
You may access my website and watch a webinar at www.ilcellulartherapy.com
Tags: arthritis, bone marrow, Celling, cellular orthopedics, Growth Factors, Hip pain, International Orthopedics Foundation, joint pain, knee arthritis, knee intervention, knee pain, lipogems, Micro-Fractured Adipose, Osteoarthritis, PRP, regenerative medicine, Regenexx, stem cells, Subchondroplasty
Dec 6, 2017
On November 16, 2017, The FDA posted definitive guidelines concerning what meets minimal manipulation rules and regulations and what is accepted under the practice of medicine guidelines in the specialty of Regenerative Medicine. The FDA further restated the requirement that regenerative medicine be governed by homologous use. As I interpret the guidelines there are winners and losers:
Winners
Physicians who use compliant regenerative therapies:
- Amniotic fluid without stem cells
- Blood-derived preparations (e.g., PRP, PPP)
- Bone marrow aspirate
Losers
Physicians who use non-compliant regenerative therapies:
- Adipose tissue-derived materials obtained by enzymatic digestion
- Amniotic fluid with cells Cord blood derived materials (non-autologous treatments)
- Stem Cell Clinics that advertise about using amniotic fluid as a source of stem cells and regenerative therapy along with those clinics that treat everything from alopecia to ALS to arthritis
You might ask how is that different from the current situation? First of all, the FDA Commissioner has stated in press releases that the FDA is going to go after bad actors. The Cures Act provided for increased funding to the FDA, which we suspect the Commissioner will use in part to go after the bad actors. Also, the FDA wrote in their Guidance on Minimal Manipulation and Homologous Use that “healthcare providers” need to pay attention. We have never seen them explicitly refer to the doctors and clinics providing regenerative medicine. Finally, the FDA indicated that there would be a transition period (3 years) during which manufacturers would need to enter the RMAT program to get their non-compliant products properly approved; or else. And the reason that there could be teeth in the “or else” is that the FDA will get lots of fees from all of the non-compliant products entering the RMAT program.
Last of all, what the FDA did not address as part of consumer protection; but what I incorporate in my daily practice is evidence based intervention.
Now that you are better informed and have an idea as to the laws governing our regenerative medicine marketplace, stay away from the Charlatans and Camp Followers. Then take the next step and ask your physician for the Outcomes Evidence on which a regenerative intervention for your arthritic joint is based before undergoing a procedure. To better understand that evidence call for (312) 475 1893 to set up a consultation
You may watch my webinar by accessing my web site www.ilcellulartherapy.com.
* Minimal Manipulation and Homologous Use
Tags: adipose tissue, Bone Marrow Concentrate, Clinical Studies, Clinical Trial. Mitchell B. Sheinkop, FDA, Hip Replacement, Interventional Orthopedics, joint replacement, Mesenchymal Stem Cell, Minimal Manipulation and Homologous Use, Orthopedic Care, Orthopedic Surgeon, Platelet Rich Plasma, PRP, regenerative therapies, stem cells