Sep 27, 2018
Until 2002, the patient seeking a joint replacement consultation would ask me “how long will new joint last”? Then came the era of minimally invasive surgery -I played a major role in the introduction-and now the question became “how long is the incision?” and “how long will I stay in the hospital?” While the number of “Regenerative Medicine” options for the treatment of osteoarthritis continues to increase, in the current medical marketplace, it is via direct to consumer advertising that “breakthroughs” are brought to the attention of those impacted by the symptoms and limitations of Degenerative Joint Disease. Whereas patients historically would base their personal medial decision making on consultation and guidance from the medical community, such is no longer the case. Media marketing is now the primary reason a patient makes the decision for which Regenerative option to choose. The problem is there is little if any scientific evidence to support the ad claims. In the one or two approaches where there is a paucity of evidence, the latter is on a handful of subjects at less than six months. Witness the recent reversal on insurance reimbursement for several placental derived products because of the absence of benefit at six months in clinical trials.
Included among the reasons featured in ads promoting Stem cells for arthritis, you will find,” it worked for me”. More recently it is a product that “recruits” your Stem Cells. On it goes with promotions for Stem Cells in cord blood, Stem Cells in Wharton’s Jelly, and Stem cells derived from your adipose tissue (fat). Missing from the entire marketing campaign in almost every scenario is outcomes data. I am an orthopedic surgeon who, prior to my Cellular Orthopedic initiative, played a major role in joint replacement surgery as Professor of Orthopedics and head of a prominent joint replacement program at a large Medical Center in Chicago. While performing clinical trials with new generations of hip and knee implants, it was well accepted in the orthopedic community that a minimum of two year follow up would be required before a scientific paper would be considered for publication. When I entered the emerging specialty of Cellular Orthopedics, I continued the integration of clinical practice with clinical research so that my interventional recommendations would be evidence based. Below are two of the manuscripts I co-authored; one having been accepted for publication and the other recently submitted for publication.
Safety and Efficacy of Percutaneous Injection of Lipogems Micro fragmented Adipose Tissue for Severe Osteoarthritic Knees
A Specific Protocol of Autologous Bone Marrow Concentrate and Platelet Products Versus Exercise Therapy for Symptomatic Knee Osteoarthritis: A Randomized Controlled Trial with 2 Year Follow-Up
What I won’t promote is anything wherein there is not two years minimum of evidence concerning safety, efficacy and satisfactory clinical outcomes. I am not opposed to progress but best practices demand clinical trials of new options and those trials should be underwritten by the pharmaceutical company; not by a patient paying relatively large sums without meeting inclusion criteria and without follow-up leading to minimum two-year outcomes evidence.
To learn more, schedule an appointment (312) 475-1893. You may visit my website www.Sheinkopmd.com
Tags: adipose tissue, Bone Marrow Concentrate, cellular orthopedic, lipogems, OA, PRP, stem cells

Sep 17, 2018
Seems strange that I would start thinking about the upcoming winter season but conditioning is sports specific and it will take about eight weeks to get ready. This past weekend, I increased my conditioning program with more cycling and strength training. It is now about nine months since I underwent cellular orthopedic interventions to both on my knees followed by both of my hips. The results have been most gratifying allowing me to extend my recreational lifestyle indefinitely; so here I am planning ahead for the upcoming ski season even though the Chicago temperature prediction is for a high of 87 degrees. Last year at this time, I questioned whether my skiing days were over. The reasoning behind much of my autobiographical, recreational subject matter is so the reader will better understand what is possible through stem cell, growth factor and platelet intervention for those with pain and limitations inherent in osteoarthritis. While an orthopedic surgeon does not need to break his or her own bones to better enable that surgeon to treat a fracture, given the number of clinics now advertising stem cell treatment, the patient choosing a regenerative medicine provider might take note of the fact that not only have I been playing a prominent role in the evolution of this expanding specialty of Cellular Orthopedics by introducing evidence based care over five years ago, I can tell you what works best from the standpoint of a patient.
There is an ever-increasing number of good and some excellent outcomes logged into our database. To be quite frank, there are some who have not fared as well. By continued surveillance and monitoring of outcomes, I am able to identify those who would improve their results by some means of augmentation be it a Platelet Rich Plasma follow-up or a repeat stem cells intervention. Let me paraphrase a message received from a patient in whose knees I have completed several cellular orthopedic interventions over the past three years. This mid 50s farmer is back to regularly playing age related group basketball several evenings each without limitation and without recurrence of symptoms the following day. Concerning yet another patient, this one in his early 90s from a patient who happens to be a family acquaintance, “I watched your patient painting the side of his garage the other day.”
Yes, these are anecdotes and so is my story; however, I think you get the message.
To learn more, you may call (312) 475-1893 to schedule a consultation. Access my web site at www.sheinkopmd.com.
Tags: cellular orthopedics, chicago, Osteoarthritis, Plate Rich Plasma, regenerative medicine, stem cells

Jul 26, 2018
Hip osteoarthritis (OA) exerts a significant burden on society, affecting 3% of Americans aged >30 years. Recent advances in the understanding of the pathoanatomy and pathomechanics of the hip have led to treatment options for young adults with hip pain. Femoroacetabular impingement, specifically cam-type femoroacetabular impingement, hip dysplasia, and the sequelae of pediatric hip disease can predispose the hip to early OA. However, many patients with abnormal anatomic findings do not develop early OA, suggesting that there exist other patient characteristics that are protective despite abnormal bony anatomy. Outcome studies show that arthroscopic and open hip procedures improve pain and function in patients with symptomatic hips. However, there is currently limited evidence that these procedures extend the life of the patient’s natural hip. Additional studies are needed to determine protective or adaptive factors in patients with abnormal anatomy who do not develop early OA and to determine whether joint preserving hip surgery extends the life of the native hip joint.
Review Article:Natural History of Structural Hip Abnormalities and the Potential for Hip Preservation
James D. Wylie, Christopher L. Peters, Stephen Kenji Aoki
What makes the article so interesting to me is first, I played a role in training one of the authors in my earlier academic career. More important is the role I am now playing in helping to preserve the life of the hip joint with a needle instead of a knife and extending the life of the “native hip joint”. The latter is done via Cellular Orthopedics. By introducing Stem Cells, Platelets, Precursor Cells, and Growth Factors, I am now able to address arthritis at a Bio-Immune level, possibly regenerate cartilage, potentially influence healing of the torn acetabular labrum, certainly reverse the secondary inflammation and thereby diminish pain and improve function in the abnormal hip joint.
It takes an evaluation in my office including the history, a physical examination and my review of your hip images after which I am able to customize the Cellular Orthopedic intervention that will help with joint preservation and potentially, joint regeneration. Our Outcomes studies continue and it is the result of ongoing data collection that allows me to extend the life of your native hip. Call (312) 475 1893 to schedule a consultation. You may visit my web site at www.sheinkopmd.com
Tags: cellular orthopedics, Dysplasia, Hip osteoarthritis, Hip pain, hip surgery, platelets, stem cells, torn labrum
Jul 19, 2018
The argument frequently advanced by orthopedic surgeons in response to a patient’s inquiry concerning stem cells for arthritis is that it is too early, there is not enough research, It is better to have a major surgical procedure. For those of you who have read my blog or have sought orthopedic consultation in my office, I have emphasized that my recommendations are evidence based. Each patient, for whom I have completed a cellular orthopedic intervention for arthritis, has been entered into a registry or clinical outcomes data base, IRB approved. Just as I pioneered the integration of clinical care with clinical research over 37 years as a joint replacement surgeon, so too do I now partake in the growth and development of the clinical pathways for regenerative medicine.
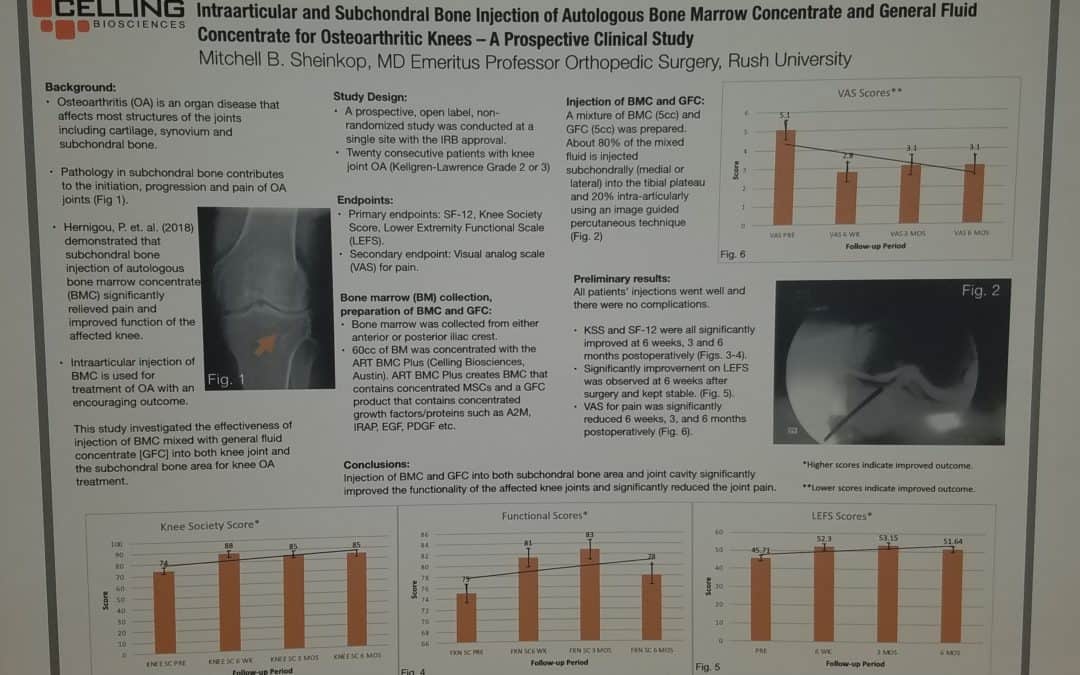
Last month, I exhibited a poster at a large regenerative medicine meeting wherein I shared my preliminary outcomes and thus educated other professionals using Intraarticular and Subchondral Bone Injection of Autologous Bone Marrow Concentrate and General Fluid Concentrate for Osteoarthritic Knees-A Prospective Clinical Study. Osteoarthritis is an organ disease that affects most structures of joints including cartilage, synovium and subchondral bone. Pathology in subchondral bone contributes to the initiation, progression and pain of Osteoarthritis. In previous European studies, the injection of autologous bone marrow concentrates into bone supporting the joint significantly relieved pain and improved function of the affected knee. The preliminary outcomes in the study that I presented via a poster exhibit, investigated the effectiveness of injections of Bone Marrow Concentrate with General Fluid Concentrate (Growth factors), into both the knee joint and the subchondral bone. The study recorded all the standard Endpoints I had previously used in joint replacement clinical outcomes trials.
Bone Marrow was collected from the pelvis and a filtration system allowed for concentration of Mesenchymal Stem Cells, Platelets, Precursor Cells and Growth factors such as A2M, IRAP, EGF, PDGF, TNF-B blocker, etc. After preparation, a mixture of Bone Marrow Concentrate and Growth factor Concentrate was injected into the bone (subchondral) and into the joint.
In the study, all patient injections went well and there were no complications. The Preliminary Results documented diminished pain and improved function. We concluded that injection of Bone Marrow Concentrate and Growth factor Concentrate into both the subchondral bone area and joint cavity significantly improved function of the affected knee joints and significantly reduced joint pain. While there are many stem cell providers to be found because of their marketing, choose the center of excellence in Cellular Orthopedics that is evidence based.
Call to schedule a scientific based consultation from an orthopedic surgeon 1 (312) 475-1893.
You may access my web site at www.SheinkopMD.com.
Tags: avascular necrosis, bone lession, bone marrow, Cartilage, cellular orthopedics, clinical study, Growth Factors, IRAP, joint pain, joint replacement, knee pain, knee replacement, meniscus tear, Osteoarthritis, platelets, PRP, regenerative medicine, sports medicine, stem cells, subchondral bone
Jul 12, 2018
Just as I cringe when a new patient announces that they have “bone on bone”, so too do I squirm when I am told by a patient “I have a torn” at times meniscus or cartilage; others, a torn rotator cuff; and then again, a torn labrum. Attention please, your X-ray or MRI image is not causing pain, the inflammation in or around your joint is the pain generator. 95% of the population over age 45 will have an abnormality interpreted by the radiologist on the report their MRI, be it of the shoulder, hip or knee. Cartilage and meniscal changes at the knee, labral tears at the hip or shoulder, and rotator cuff abnormalities are part of the attritional process; alternatively, these changes are commonly over diagnosed.
Last week, a 70-year-old woman called to schedule an appointment and indicated that she had a torn acetabular(hip) labrum diagnosed on a recent MRI. I responded, “your pain generator is arthritis unless you are a hockey goalie”. I was being a bit facetious but at the same time truthful. My 37-year experience as a reconstructive orthopedic surgeon specializing in hip and knee replacement really prepared me for this life after surgery; namely, a cellular orthopedic interventionalist.
It takes a history and hands on physical examination prior to review of images to determine what is causing a painful musculoskeletal condition. The common denominator is inflammation, not a computer image. In the case of arthritis, unless the cartilage (meniscus), labrum or rotator cuff alteration is generating mechanical problems such as weakness, locking, “clunking” or giving way, we frequently need not address the former with a maximally invasive surgical procedure; a needle will suffice and deliver the platelets, Mesenchymal Stem Cells, Growth Factors and precursor cells required to address pain, improve function, increase motion, stop progression of arthritis and restore, at times regenerate the joint.
Cellular Orthopedics encompasses a full joint Preservation, Restoration and Regenerative scope of options. The notion introduced by a print media ad, that it is “one and done”, won’t help you postpone, perhaps avoid a joint replacement. In my practice, we monitor progress and intervene when necessary at five months or five years if indicated.
To learn more, visit my web site at www.SheinkopMD.com or call and schedule a consultation at (312) 475-1893
Tags: arthritis, bone lesion, Bone Marrow Concentrate, cellular orthopedics, hip pian, joint pain, joint replace, knee pain, meniscus, Osteoarthritis, PRP, Rotator cuff, stem cells, stiffness, torn labrum