
Jan 16, 2019
I swear to tell the truth, the whole truth, so help me G_d. Injured cartilage in a skeletally mature adult typically doesn’t heal on its own; surgical techniques are needed in an attempt to repair and replace cartilage. These latter procedures are appropriate for specific cartilage injury, rather than the widespread cartilage changes found in the osteoarthritic joint. That is not to say that someday soon, we may have the ability to regenerate cartilage. Research is ongoing in regenerative medicine with continual progress as evidenced by preliminary success in spinal cord injured patients:
StemCyte gets FDA green light to continue studying spinal cord injury treatment stem cells.
Now for the bad news. In spite of false news generated by the charlatans, parasites, camp followers and hucksters in their Regenerative Medicine seminars, print media and television adds; there is no scientific evidence to support their claims of cartilage regeneration, hair restoration, cure of erectile dysfunction, so on and so forth.
Stem cell fraud? Couple says therapy gave them ‘false hope’
“Unfortunately, what I had hoped to be a hard-hitting expose turned into limp-noodle babbling. Another missed opportunity.” Continuing the commentary about regenerative medicine clinic charlatans and fraud started by NBC, when a patient showed me a brochure from yet another group that holds itself out to treat every abnormal medical condition from A to Z with “Stem Cells”, I suggested that he request data regarding their successes. Please bear in mind the self- contradicting adage that Always and Never statements are always false and never true. They are frequently used by people who suffer from personality disorders. On Friday he sent me the response to his inquiry regarding outcomes at a one of the national stem cell clinics.
“success rates per our clinical research network are VERY encouraging: Orthopedic: knee 83%, hip 80%, back (cervical, thoracic, lumbar, sacral 80% ave., ED 77%, Cataracts 100%” Remember what I just wrote about Always and Never?
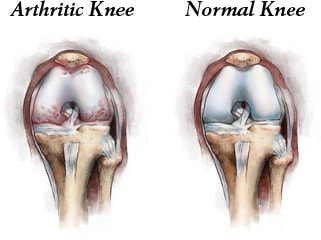
The good news though is that there is emerging scientific evidence to justify Joint Restoration with a cellular orthopedic procedure. While an image of an arthritic joint allows for identification of cartilage and meniscal changes, that same image will frequently be consistent with bone marrow edema, and thickening of the bone adjacent to a joint (subchondral sclerosis) as well as loose bodies within the joint. As cartilage does not have a nerve supply, the pain generation in Osteoarthritis more probable than not is the result of inflammation of the synovial joint lining and the subchondral bone. While there is no scientific means of re-growing cartilage after age 40 at this time-defects may be filled by surgery-orthopedic surgeons focusing on Cellular Orthopedics have developed methods to restore the joint function by blocking the pain generators, restoring healthy subchondral bone, and reversing bone marrow edema.
To schedule an Evidence Based Consultation, call (312) 475-1893
You may read my Blog and explore my published research articles on the website www.sheinkopmd.com
Tags: arthritis, bone marrow edema, cartilage regeneration, cellular orthopedic, Hip pain, inflammation, joint health, joint pain, knee pain, medicine, meniscus tear, Osteoarthritis, restoration, soft tissue repair, stem cell, stem cell injection, subchondral bone

Nov 19, 2018
“THE GOOD NEWS IS THAT MY 80-YEAR-OLD TEAM ‘CHICAGO GEEZERS’ WON THE WINTER NATIONALS FOR OUR AGE GROUP IN FT MYERS 11/6 – 11/8. I RAN FOR MYSELF AND HIT .710. THE BAD NEWS IS MY LEFT KNEE IS A BIT MORE ACHY NOW, EVEN WHEN I AM SLEEPING OR NOT PLAYING SOFTBALL. IT IS NOT REALLY PAINFUL BUT IT DOES ACHE MORE THAN IT USED TO. HOPEFULLY, AFTER A FEW MORE MONTHS WE WILL NOTICE A REAL IMPROVEMENT” J.H.
While growing up in Albany Park, 16-inch softball was a way of life starting at the Haugan Grammar School playground in early February and continuing until the football season in the late fall while basketball went on all year round. Weather permitting, we relocated to Jensen Park and later during high school years to Eugene Field Park, River Park and eventually the Hibbard School Yard. Softball teams with such names as the Torpedoes, Majestics, Olympians, Phaetons, Regular Fellows, Little Gents, Jovens, and Aristocrats, to name a few, competed for the highly coveted Ned Singer softball championship. Teams were comprised of teenagers representing Amundsen, Austin, Roosevelt Sullivan, Senn, Von Steuben High Schools and more. The soft ball leagues diminished in numbers after high school but several individuals continued playing wherever and whenever possible. I for one played until age 40, ending my career with a triple play and fractured finger at Union Park in the Hospital league. A new 16-inch clincher is hard as rock. There are few remaining players of that generation; I am privileged to serve as a treating physician to two. Jimmy, someone I met when he beat out a ground ball over 00 years ago, (I was a first baseman) practices law and continues to play. Though he had overcome many softball related injuries during his playing days, he was ready to quit three or four years ago out of embarrassment at the pinch runner until I intervened with a Cellular Orthopedic intervention and he regained the ability to beat out a ground ball. Jerry, middle row in the photo, second from the left, continues to play. Two years ago, also very concerned about his ability to run around the bases, he presented to my office seeking an alternative to a Total Knee Replacement for his arthritic knees. One picture says it all; he is already making plans for next year. In Jerry’s case, it took several biologic interventions; but he is a champion.
To schedule an appointment and learn about the biologic options for your joints call (312) 475-1893. You may visit my web site at www.Sheinkopmd.com.
Tags: arthritic knee, biologic intervention, cellular orthopedic, injection, joint pain, joint replacement, Orthopedic Surgeon, PRP, regenerative medicine, stem cell, Total Knee Replacement
Oct 18, 2018
We are speaking of stem cell therapy integrated with clinical research, and the resultant evidence-based stem cell intervention. Osteoarthritis is becoming more prevalent as I am seeing younger patients with arthritis as a consequence of sporting injuries such as ACL tears. The baby boomer population is experiencing accelerated onset of arthritis; their joints are prematurely aging in large numbers. At the same time, the master population is aging and living longer. As a result, I continually research biologic interventions to best address the ever-increasing number of those effected.
Why should a patient choose an orthopedic surgeon to manage their Osteoarthritic related symptoms and functional impairment? Our world is evidence based.
Study Observes Better Outcomes for OA Patients Treated by an Orthopaedic Specialist
In a retrospective study published online in BMC Musculoskeletal Disorders, shoulder osteoarthritis (OA) patients received faster and more invasive treatment when they received a new diagnosis from an orthopaedic specialist (OS) versus a nonorthopaedic physician (NOP). Patients with shoulder OA (n = 572) received care from either an OS (n = 474) or NOP (n = 98) on the date of their index shoulder visit. OS patients received their first treatment significantly quicker than the NOP cohort (16.3 days versus 32.3 days, respectively). The OS group also had higher rates of operative treatment within one year following their initial visit.
Study: Patients Report Similar Improvements for Nonobstructive Meniscal Tear with PT and Early Surgery
Physical therapy (PT) may not be inferior to early operative treatment of arthroscopic partial meniscectomy (APM) for improving knee functionality in patients with nonobstructive meniscal tears, according to a study published online inJAMA. The randomized clinical trial included 321 patients with nonobstructive meniscal tears aged 45 to 70 years who were treated at nine hospitals in the Netherlands between July 17, 2013, and Nov. 4, 2015. Patients were treated with APM (n = 159) or a predefined PT protocol (n = 162) that included 16 exercise therapy sessions over eight weeks. PT sessions focused on coordination and closed kinetic chain strength exercises. At 24-month follow-up, knee functionality in the PT group improved by 20.4 points compared to 26.2 points in the APM group. The difference did not exceed the noninferiority margin.
In order to maximize the benefits, Orthobiologics, that is stem cell therapy must be integrated with clinical research, and the resultant evidence-based stem cell intervention followed long term. In my practice, I am researching biologic interventions to address the ever-increasing number of those effected, not one and done. To learn more or schedule a consultation, Call (312)475-1893. You may visit my web site and read my blogs at www.sheinkopmd.com
Tags: ACL tear, arthritis, Cartilage, cellular orthopedic, joint pain, joint replacement, knee pain, MCL tear, meniscus tear, menisectomy, orthobiologics, orthopedic surgen, Osteoarthritis, Physical Therapy, PRP, regenerative medicine, stem cell
Sep 27, 2018
Until 2002, the patient seeking a joint replacement consultation would ask me “how long will new joint last”? Then came the era of minimally invasive surgery -I played a major role in the introduction-and now the question became “how long is the incision?” and “how long will I stay in the hospital?” While the number of “Regenerative Medicine” options for the treatment of osteoarthritis continues to increase, in the current medical marketplace, it is via direct to consumer advertising that “breakthroughs” are brought to the attention of those impacted by the symptoms and limitations of Degenerative Joint Disease. Whereas patients historically would base their personal medial decision making on consultation and guidance from the medical community, such is no longer the case. Media marketing is now the primary reason a patient makes the decision for which Regenerative option to choose. The problem is there is little if any scientific evidence to support the ad claims. In the one or two approaches where there is a paucity of evidence, the latter is on a handful of subjects at less than six months. Witness the recent reversal on insurance reimbursement for several placental derived products because of the absence of benefit at six months in clinical trials.
Included among the reasons featured in ads promoting Stem cells for arthritis, you will find,” it worked for me”. More recently it is a product that “recruits” your Stem Cells. On it goes with promotions for Stem Cells in cord blood, Stem Cells in Wharton’s Jelly, and Stem cells derived from your adipose tissue (fat). Missing from the entire marketing campaign in almost every scenario is outcomes data. I am an orthopedic surgeon who, prior to my Cellular Orthopedic initiative, played a major role in joint replacement surgery as Professor of Orthopedics and head of a prominent joint replacement program at a large Medical Center in Chicago. While performing clinical trials with new generations of hip and knee implants, it was well accepted in the orthopedic community that a minimum of two year follow up would be required before a scientific paper would be considered for publication. When I entered the emerging specialty of Cellular Orthopedics, I continued the integration of clinical practice with clinical research so that my interventional recommendations would be evidence based. Below are two of the manuscripts I co-authored; one having been accepted for publication and the other recently submitted for publication.
Safety and Efficacy of Percutaneous Injection of Lipogems Micro fragmented Adipose Tissue for Severe Osteoarthritic Knees
A Specific Protocol of Autologous Bone Marrow Concentrate and Platelet Products Versus Exercise Therapy for Symptomatic Knee Osteoarthritis: A Randomized Controlled Trial with 2 Year Follow-Up
What I won’t promote is anything wherein there is not two years minimum of evidence concerning safety, efficacy and satisfactory clinical outcomes. I am not opposed to progress but best practices demand clinical trials of new options and those trials should be underwritten by the pharmaceutical company; not by a patient paying relatively large sums without meeting inclusion criteria and without follow-up leading to minimum two-year outcomes evidence.
To learn more, schedule an appointment (312) 475-1893. You may visit my website www.Sheinkopmd.com
Tags: adipose tissue, Bone Marrow Concentrate, cellular orthopedic, lipogems, OA, PRP, stem cells

Aug 30, 2018
Evidence for the efficacy of Platelet Rich Plasma, a blood-derived formulation, and bone marrow derived biologics in osteoarthritis continues to grow in the orthopedic community. On the other hand, as I continually monitor the current landscape of indiscriminate and sometimes inappropriate marketing and use of biologics by the non-orthopedic opportunists, I doubt if the charlatans and camp followers have an overview of what is known about these agents. The increased presence of clinics Is driven by the popularity of PRP and its biologic cousins:
- consumer demand
- aggressive marketing
- a low regulatory bar for many of these regenerative medicine clinics
- the autologous nature that makes many approaches largely safe
- positive data from centers such as ours demonstrating functional and symptom modification
PRP works by activating cellular pathways; more than 3,000 genes are related to these and other pathways, suggesting that PRP probably acts by inducing a transitory inflammatory event, which then triggers tissue regeneration. Bone Marrow Concentrate, does more and addresses the subchondral bone when appropriately injected as well as initiate joint preservation and possible regeneration.
Taking aim
I use a hemoanalyzer to characterize a dose of PRP or Bone Marrow Concentrate allowing me to quantify the composition and biologic activity of these agents. Soon, I will begin pretreatment assessment of the synovial fluid of the arthritic joint so as to best determine who is the optimal candidate for a particular procedure
What do we know?
- Knee osteoarthritis: white blood cell-poor PRP has a positive effect on symptoms, not structure; while Bone marrow Concentrate affects symptoms and structure. I identify what I am putting into the patient. My goal is to have reliable predictors of outcome; that is, do the composition and biologic activity of the material implanted in the patient predict the clinical/imaging outcomes? My PRP contains a high concentration of anti-inflammatory cytokines and anabolic growth factors whereas my use of Bone Marrow Concentrate inside the bone adjacent to the joint in addition to the joint itself is improving the outcomes of the patients I treat.
- To learn more, call my office to schedule an appointment at (312) 475-1893
- You may view my Web site at WWW.Sheinkopmd.com
Tags: anit-inflammatory, biologics, bone marrow, cellular orthopedic, cellular therapy, cytokines, knee osteoarthritis, Orthopedic Surgeon, PRP, regenerative medicine, stem cell